Potassium sparing diuretics – Mechanism and actions
by egpat 08 Apr 2020
Normally we know the diuretics like FUROSEMIDE and chlorthiazide that increase the excretion of sodium along with other ions like calcium and potassium. So when these drugs are used they may cause loss of potassium resulting in hypokalemia which is sometimes fatal. But, is there any drug that increases sodium excretion at the same time retains potassium? Yes, we have one category of drugs called potassium sparing diuretics that do this job.
So here let’s see different types of potassium sparing diuretics and how they act? Interestingly all these potassium sparing diuretics act the collecting tubule of the nephron. Before going to details of these drugs directly, first of let’s see what is the role of collecting tubules in controlling potassium levels and how it can be targeted by these drugs.
Role of collecting tubules
After the glomerular filtration, the filtrate is passed through different parts of the nephron such as proximal convoluted tubule, loop of henle, distal tubule and finally to the collecting tubules and collecting ducts. Even the location and expression of these parts of nephron are slightly different still the main purpose of these parts is same, that is, absorption of essential ions from the filtrate.
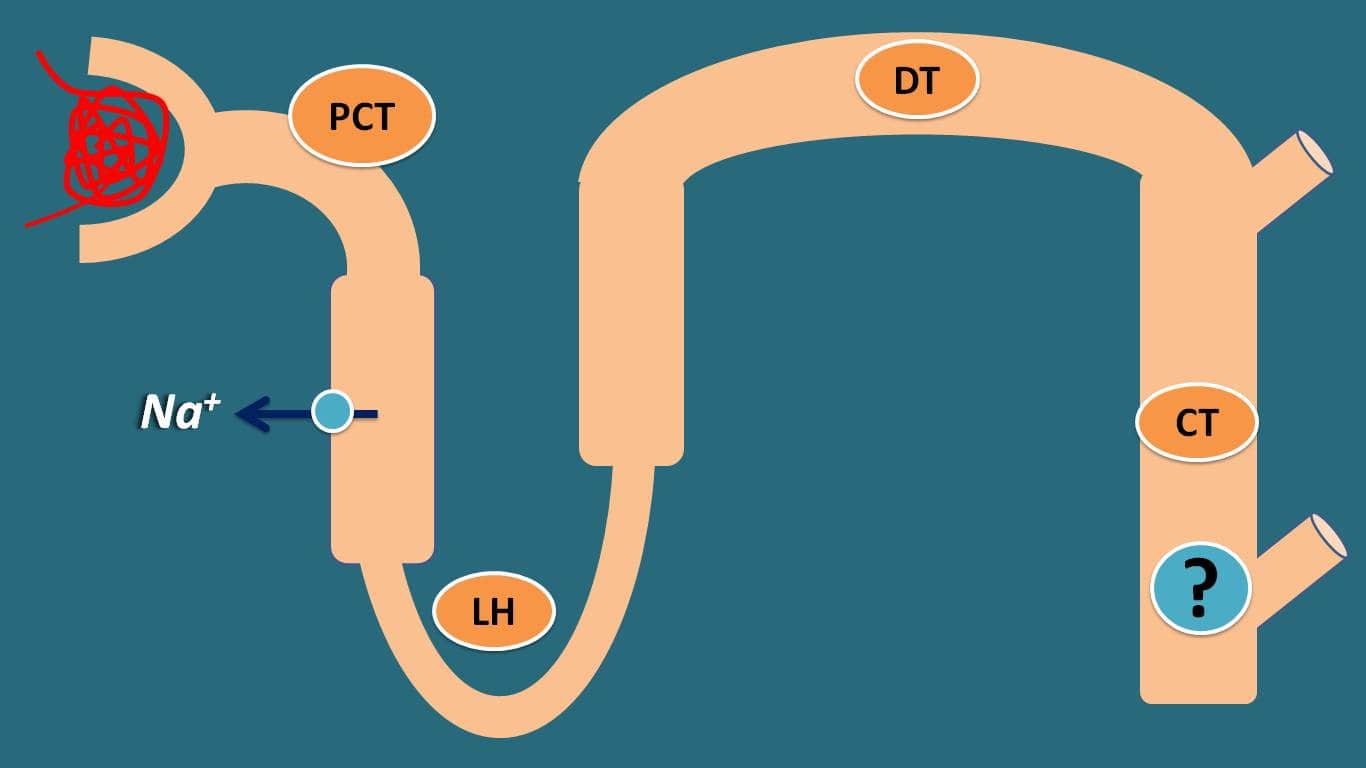
For instance, at ascending loop henle sodium is reabsorbed by Na+/K+/2Cl- pump on the apical membrane where loop diuretics act. Similarly at distal tubule, this function is mediated by another pump Na+/ Cl- exchange pump.

But at the collecting tubule, which is the terminal part of nephron, sodium should be reabsorbed according to the physiological requirements. Suppose, in the conditions like either hypotension or when sodium levels are less in the blood, then more sodium should be reabsorbed at the collecting tubule otherwise it will be lost out of the body along with urine.
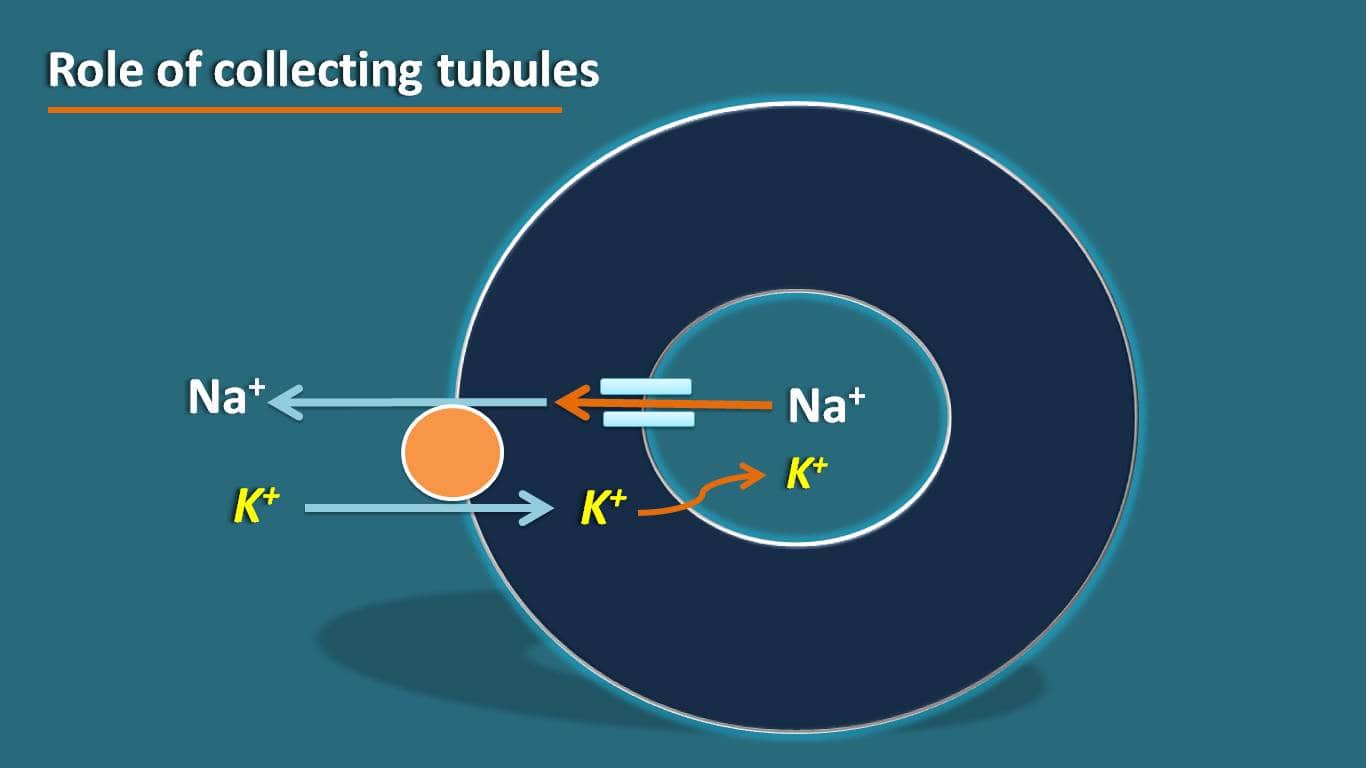
So here a specialized system is required to collect sodium into the body by reabsorption. This function is mediated by the sodium channels that are expressed on the inner membrane of the apical membrane.
But how these sodium channels are operated? As with many of the ion channels at epithelial membrane, these channels also work by concentration gradient across the membrane. Again this process should be controlled by any physiological mechanism that maintains homeostasis.
Aldosterone is one of the hormones that is released from the adrenal gland that controls the expression of the epithelial sodium channels so that the amount of sodium reabsorbed at the collecting tubules is under strict control.
Loss of potassium
We have seen that sodium is reabsorbed by the epithelial sodium channels at the collecting tubules. But what happens to the potassium? How it is related with the sodium reabsorption at the collecting tubules?
Here the role of another pump Na+/K+-ATPase pump that is expressed on the basolateral membrane comes into the picture. As the sodium is reabsorbed from the apical membrane through the ion channels, it will be transported out of the membrane into the systemic circulation by Na+/K+-ATPase pump where sodium is exchanged for potassium
In another words, sodium is reabsorbed into the systemic circulation whereas potassium is secreted into the tubules resulting in loss of potassium. So as the sodium is more reabsorbed, potassium is more lost out of the body.
That’s why loop and thiazide diuretics mainly produce hypokalemia. These categories of drugs act at loop of henle and distal tubule respectively. They inhibit sodium reabsorption at these locations so that the filtrate that reaches at collecting tubule is rich in sodium.
Now some part of the sodium is reabsorbed at the collecting tubule for exchange of potassium resulting in hypokalemia produced by these drugs.
Potassium sparing diuretics
Now we have few of the drugs like amiloride, triamterene, spironolactone and eplerenone that act the collecting tubules and inhibit the sodium reabsorption. As sodium is not reabsorbed potassium is retained within the body resulting in the potassium sparing effect.
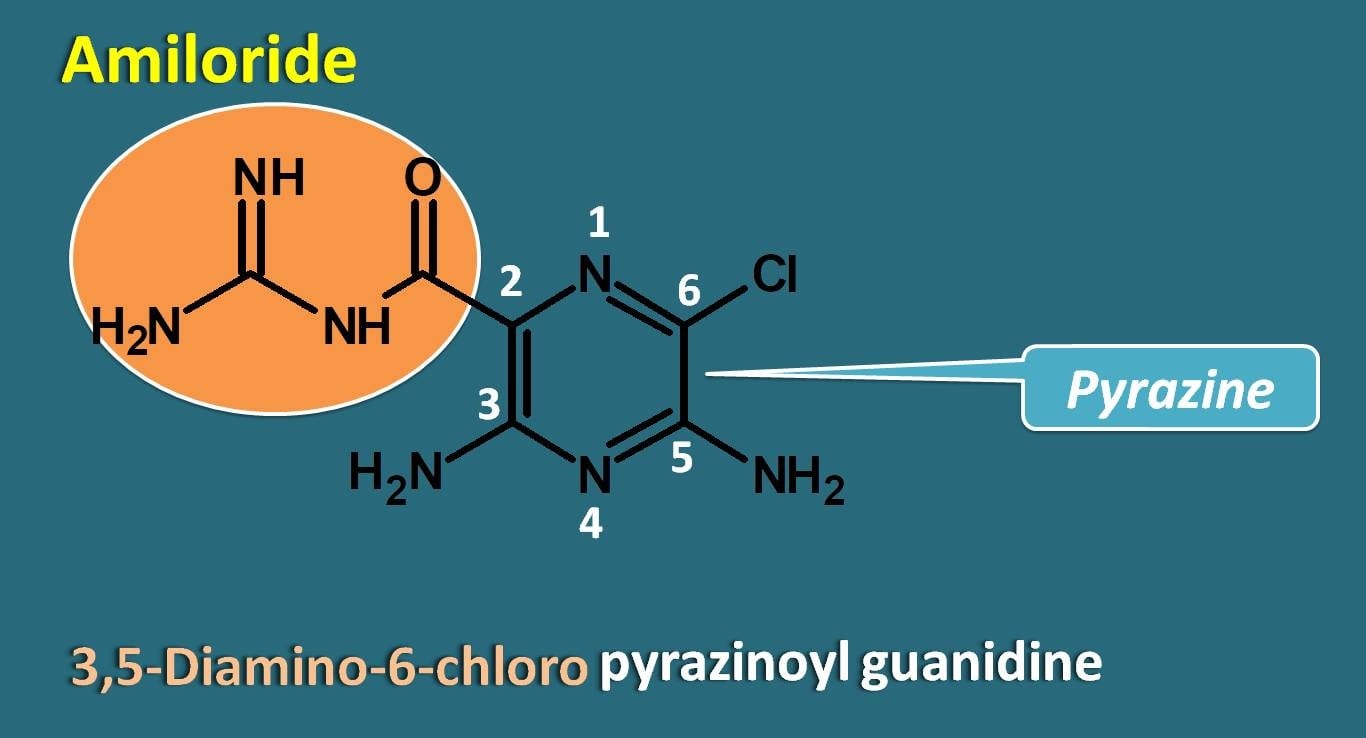
Amiloride is having pyrazine ring system that is attached with carbonyl guanidine at 2nd position. So it is a pyrazinoyl guanidine derivative with two amino groups at ,5 potions and a chlorine group at 6th position.
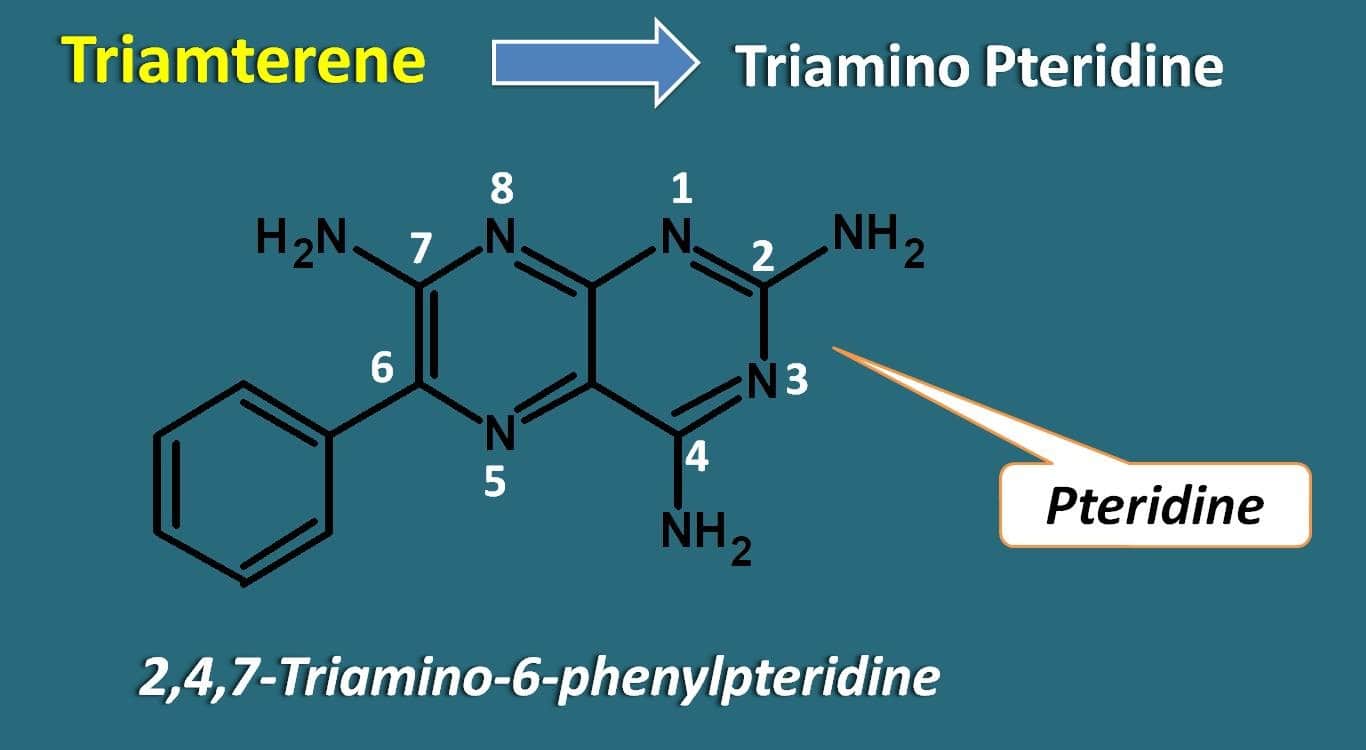
As the name itself indicates, Triamterene contains a pteredine ring with three amino groups at 2,4 and 7 positions. It also has phenyl ring attached at 6th position. So chemically it is a 2,4,7-triamino-6-phenylpteridine.
Finally we have two steroidal drugs such as spironolactone and eplerenone that are included in this category. Both of these drugs are derivatives of pregnane nucleus attached with a 5 membered lactone ring with by a spiro linkage.
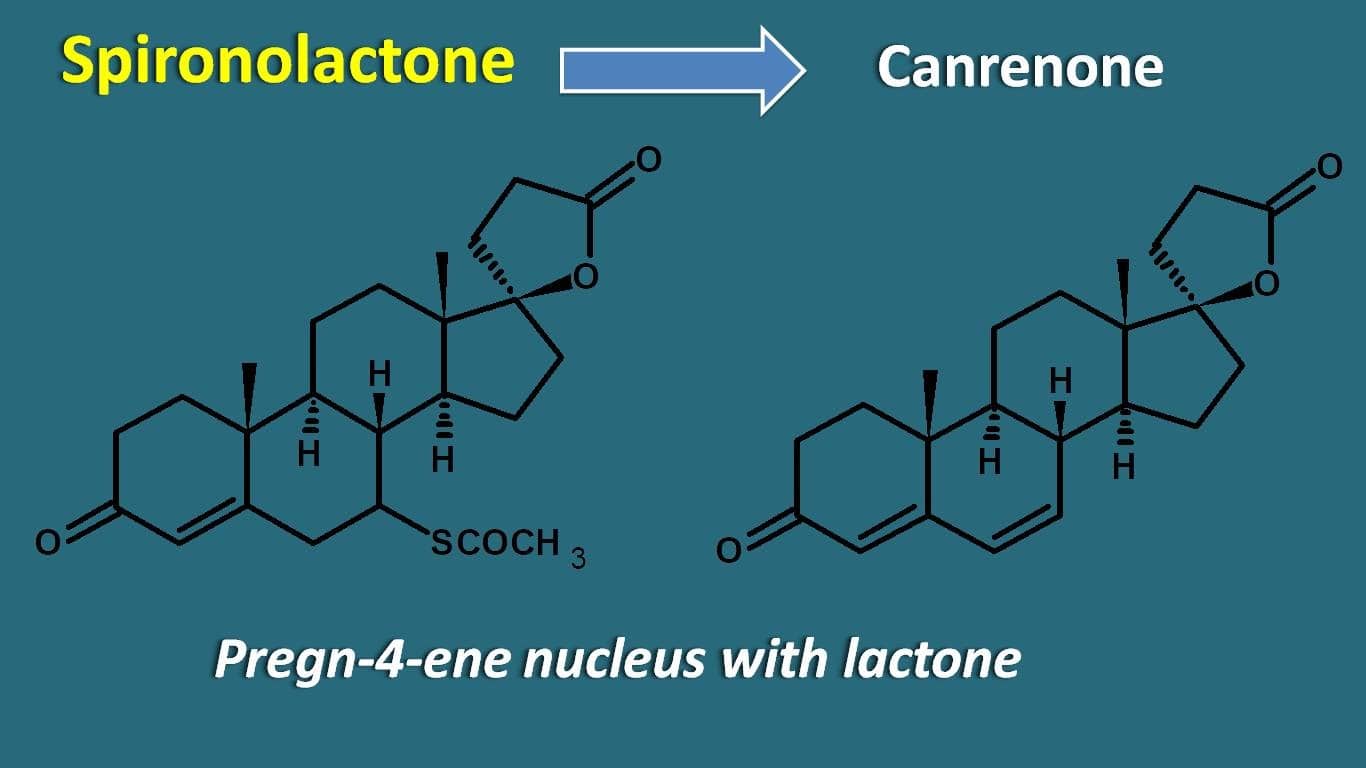
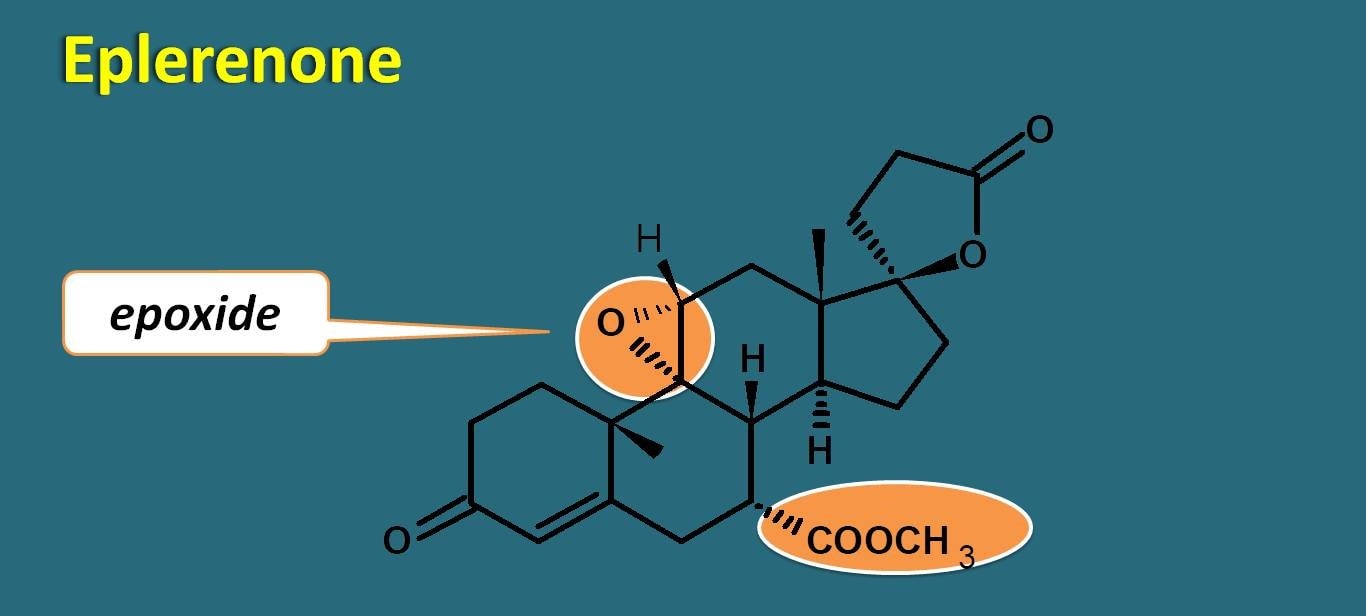
One of the metabolite of spironolactone is canrenone which is also active and sometimes used directly as potassium sparing diuretic. Eplerenone differs from spironolactone in the fact that it has an extra epoxide linkage and methyl carbamate group instead of acetyl thio group at 6th position.
How they act
But all these drugs do not act by similar mechanism. Drugs like amiloride and triamterene directly block the epithelial sodium channels thereby prevent sodium reabsorption. But these two drugs have no action at the aldosterone receptors.
On the other hand, drugs like spironolactone and eplerenone act as competitive antagonists at the aldosterone receptors thereby they prevent the action of aldosterone. Normally aldosterone acts on the mineralocoritcoid receptors which are nuclear receptors that increase gene transcription and protein synthesis.
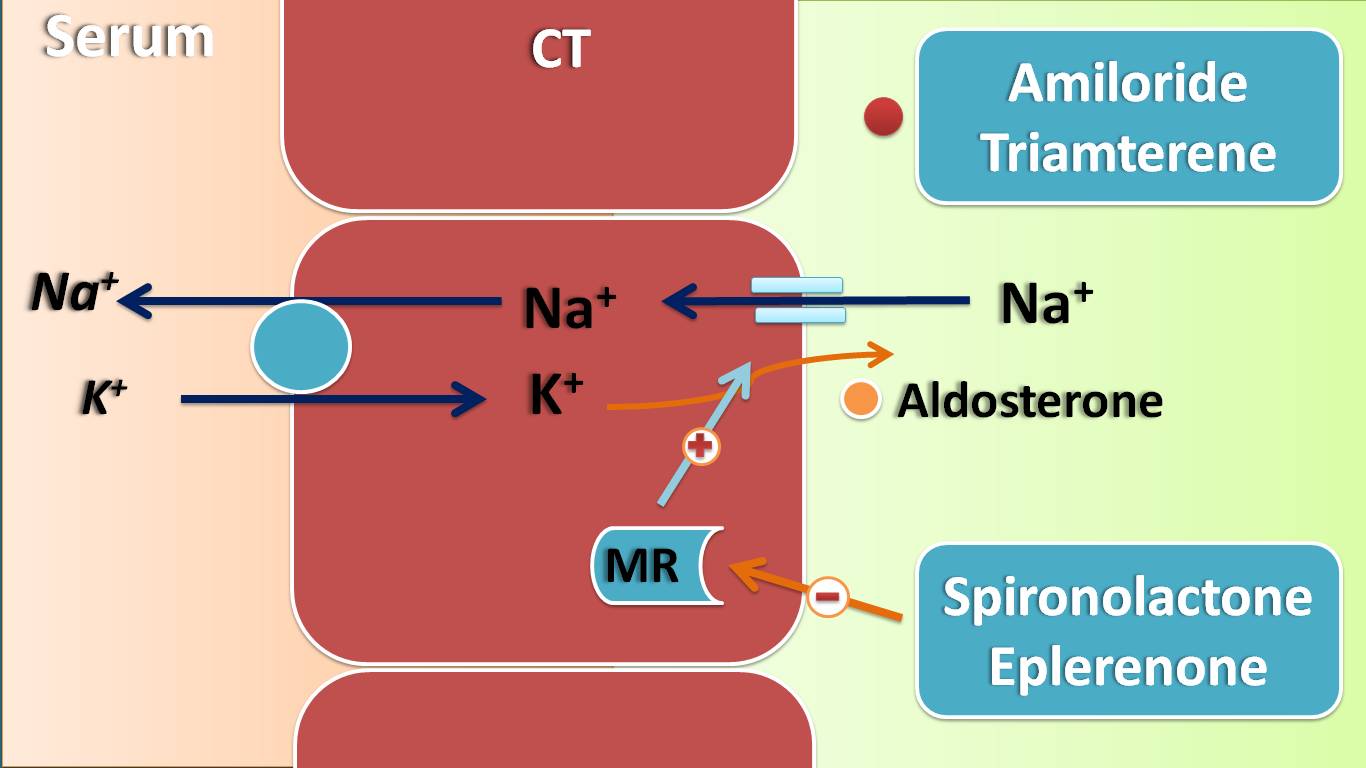
Here the proteins that are synthesized are nothing but the sodium channels which are then expressed on the apical membrane resulting in sodium reabsorption. Now spironolactone and eplerenone block these receptors thereby reduce the expression of epithelial sodium channels.
Effects on physiological system
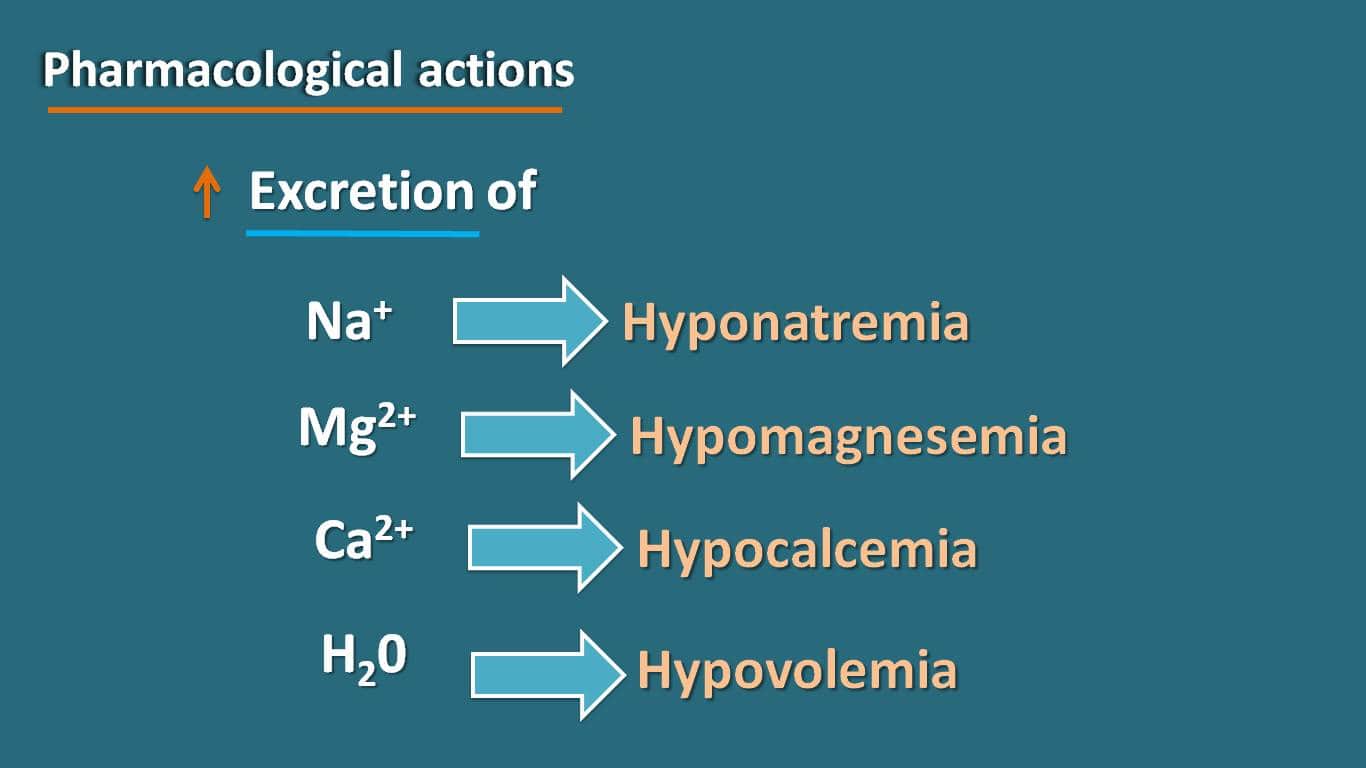
As these drugs block sodium reabsorption through the renal tubules, one of their main effects is to reduce the body volume producing hyponatremia and hypovolemia. Similar to other diuretics they increase excretion of other ions like calcium, magnesium and chlorides.
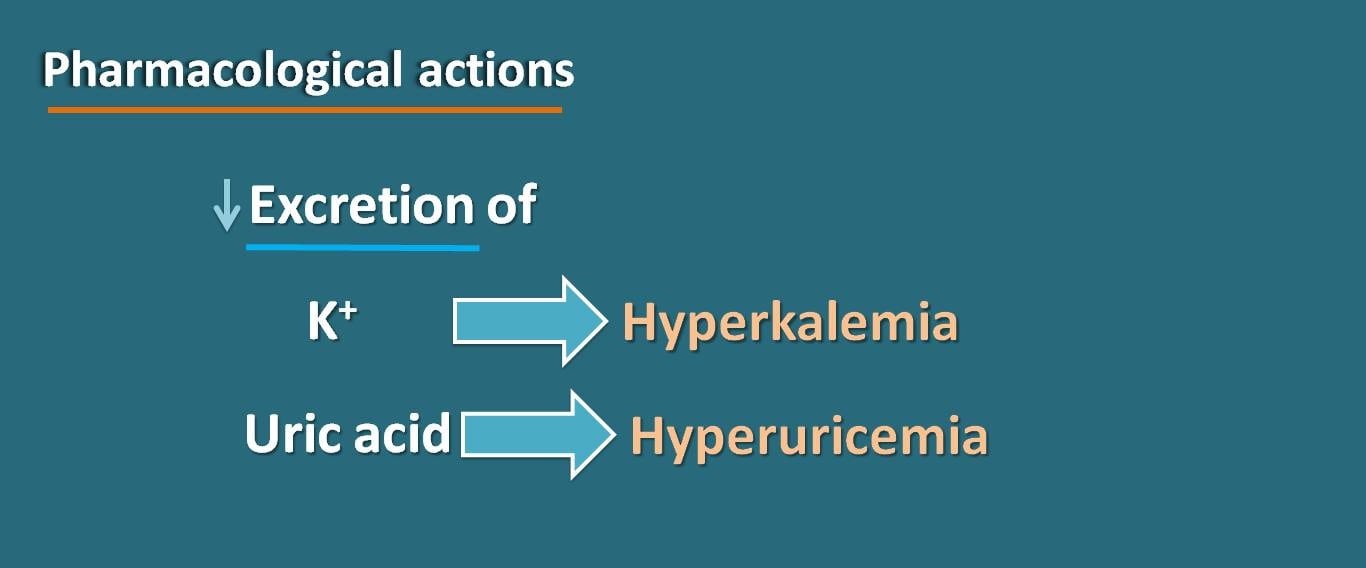
Interestingly, these drugs retain two components in filtrate. One is the potassium, due to their inhibitory action on sodium reabsorption. Second, is on the uric acid. Just like other diuretics, these drugs retain uric acid resulting in hyperuricemia.
Even most of the adverse effects of potassium sparing diuretics are related with their renal actions. These drugs can produce hyponatremia, hypotension, hypocalcemia and hypomagnesaemia as few of the side effects along with hyperkalemia and hyperuricemia.
Few of the side effects may not be related to renal actions. For example, spironolactone can produce gynaecomastia in men and menstrual irregularities, amenorrhea in women. Similarly triamterene can produce renal stones due to its poor water solubility.
Clinical uses
As the main role of these drugs is to retain the potassium, these drugs play an important role in conditions like hypokalemia that may be induced by other drugs like loop and thiazide diuretics.
These drugs can also be used in the treatment of severe form of heart failure where they reduce the body volume and thereby reduce cardiac work load. Due to the same reason, they also found useful in treatment of hypertension.
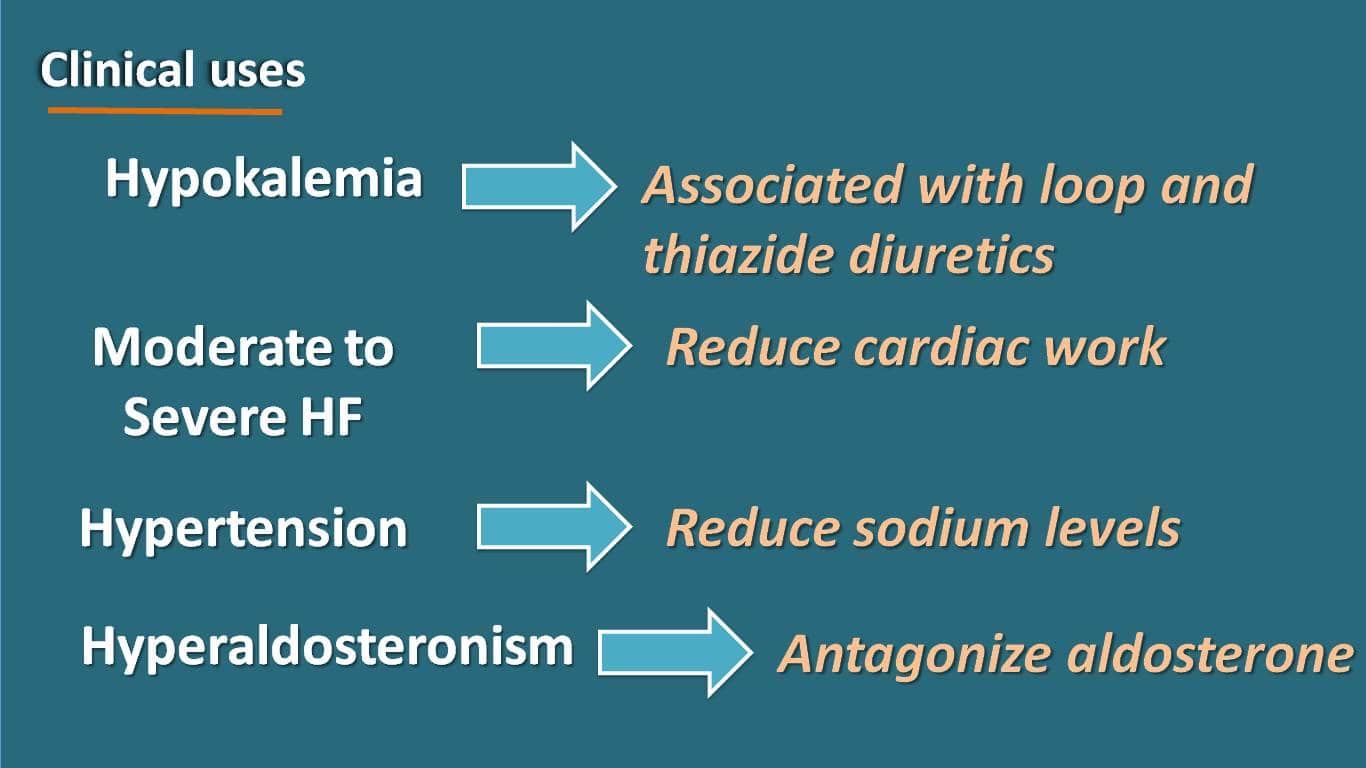
Among these drugs aldosterone antagonists like spironolactone and eplerenone can be used in primary hyperaldosteronism to antagonize the actions of aldosterone.